
The use of unnecessary interventions in labour and birth continues to rise. A rate of > 19% is seen as medically unnecessary by the World Health Organization (WHO) (Gibbons et al, 2010); in Europe, caesarean section rates vary between 30–58%, except in the Netherlands and Scandinavian countries where the rate is 16–17% (Zeitlin et al, 2013). The caesarean section rate in the UK is currently 26.2%, but wide variations of 18–34% are reported (NHS England, 2013). Morbidities associated with such interventions may have an impact on the long-term physical, mental and sexual health of women and disrupt maternal–infant relationships (Beck and Watson, 2008; Koblinsky et al, 2012; Firoz et al, 2013). Evidence that such interventions increase childhood asthma, obesity, diabetes, cancers and atopic diseases is increasing (Hyde et al, 2012; Dahlen et al, 2013).
A significant policy initiative in the UK to reduce unnecessary interventions is promoting the choice of midwife-led settings for birth. This model of care recognises women's ability to give birth with minimal intervention. A review of this policy demonstrated that interventions in obstetric-led environments are 15–25% higher among low-risk women when compared to midwife-led settings (Birthplace in England Collaborative Group, 2011). Currently, only 8% of women in the UK use midwife-led settings for birth. Efforts to increase the use of these settings are hampered by dominant discourses about birth as a risky process and medical interventions as necessary to reduce or prevent harm (Coxon et al, 2014). In this context, it is important to consider how findings of poorer neonatal outcomes among primigravid women choosing homebirths, and a transfer rate of 35–45% from midwife-led to obstetric settings, will have an impact on women's decisions (Birthplace in England Collaborative Group, 2011).
Updated National Institute for Health and Care Excellence (NICE, 2014) guidelines recommend midwife-led environments as the choice of place of birth for women with low-risk pregnancies. Improving the availability and utilisation of such environments is necessary to improve outcomes. However, the use of unnecessary interventions in obstetric environments must be addressed if women who choose these environments are to experience positive outcomes. High-risk women in such units will also benefit from normalisation (O'Connell and Downe, 2009; Kennedy et al, 2010).
Although midwife-led environments are associated with reduced intervention, it is important to consider whether improving implementation of evidence-informed skills further can reduce the rate of transfer to obstetric units. The transfer rate from freestanding midwifery units of 16.5% with better outcomes, compared to 21.2% in alongside midwifery units, suggests that there may be differences in the quality and quantity of implementation (Birthplace in England Collaborative Group, 2011). It also important to investigate whether a lack of implementation of evidence and involvement of women in decision-making has resulted in poorer outcomes among primigravid women who chose homebirth.
The strength of evidence from research investigating the reasons for differences in interventions and outcomes between birthing environments is of variable quality. However, a finding common to these studies is poor implementation of evidence and the lack of involvement of women in decision-making (O'Connell and Downe, 2009; Kennedy et al, 2010; McCourt et al, 2012; Walsh and Devane, 2012). The importance of systematically measuring care to understand these variations and improve the consistency of care and outcomes is emphasised in policies, research and investigations into midwifery practice (Kennedy et al, 2010; Stones and Arulkumaran, 2014; Alderwick et al, 2015; Kirkup, 2015).
The Keeping Birth Normal tool
This study piloted a tool to measure the implementation of evidence to reduce unnecessary interventions in labour and the first hour of birth. The validation of the Keeping Birth Normal (KBN) tool is in the developmental stage. The tool is based on a model that sees birth as a normal and healthy event, and the involvement of women as necessary to achieve positive outcomes (Department of Health (DH), 2007; Green, 2012). The care includes the first hour of birth, where risk of intervention is increased if there is a lack of skills to support the physiological birth of the placenta and promote transition of the baby to external life (Dodwell and Newburn, 2010; American College of Nurse-Midwives et al, 2012).
Several tools have been developed to measure support in labour (Ross-Davie et al, 2013; Dunne et al, 2014). Though shown to be vital to improving outcomes, this is only one measure of care described to reduce unnecessary interventions (Dodwell and Newburn, 2010; NICE, 2014). The KBN tool measures care under 12 domains and 50 items (approaches) on evidence-informed skills to support a normal birth (Table 1; Table 2).
| Twelve domains | Evidence-informed skills |
|---|---|
| 1. Philosophy | Orientation to reduce interventions |
| 2. Facilitating choice | Inclusion of women to improve outcomes |
| 3. Guidelines | Use of evidence to improve outcomes |
| 4. Partnership working and communication | Use of evidence to promote safe practice |
| 5. Environment | Supports physiological birth |
| 6. Supporting women in labour | Care that supports physiological processes to reduce interventions |
| 7. Progress in early labour | Care that supports physiological processes to reduce interventions |
| 8. Active labour | Care that supports physiological processes to reduce interventions |
| 9. Imminent birth | Care that supports physiological processes to reduce interventions |
| 10. Birth of placenta | Care that supports physiological processes to reduce interventions |
| 11. Birth of baby and breastfeeding | Care that supports physiological processes to reduce interventions |
| 12. Respecting women | Building relationships that improve outcomes |
| 2. Facilitating choice | 0 | 1 | 2 | 3 | 4 |
| 2.1. The woman's choice is the focal point of my discussions with her regarding plans for her birth | |||||
| 2.2. I am up to date on evidence to support choices in normal birth | |||||
| 2.3. I act as the woman's advocate when the woman's choice falls outside of guidelines | |||||
| 3. Guidelines | 0 | 1 | 2 | 3 | 4 |
| 3.1. I use local and national guidelines during information-giving |
Rating scale: 0 = unable to assess; 1 = rarely uses this skill; 2 = sometimes uses this skill; 3 = frequently uses this skill; 4 = consistently uses this skill
‘ The Keeping Birth Normal tool has the potential to support implementation through structured preceptorship and peer-review processes to reduce variations, promote physiological birth and improve outcomes ’
Post-validation, the KBN tool has the potential to support implementation through structured preceptorship and peer-review processes to reduce variations, promote physiological birth and improve outcomes. It can be used by midwives to provide evidence of skill development when preparing for revalidation with the Nursing and Midwifery Council (NMC). It may be considered for use by Trusts, which may be given responsibility for supervision under current changes proposed by the Government to the statutory supervision of midwives (DH, 2016).
In relation to research, the KBN tool can be used to produce more robust evidence compared to surveys and interviews, often used to study implementation (Ubbink et al, 2013). It could be used widely in the field of normal birth to measure and support the implementation of evidence, gather evidence of why interventions are reduced in some environments compared to others, measure the inclusion of women in decision-making, and potentially enable researchers to draw causal links between the use of approaches associated with reduced interventions and outcomes.
Validation
The validation of the KBN tool is informed by Kane's Interpretation and Use framework (Figure 1). This framework is based on the theory that validity is not about the properties of a tool, rather the inferences that are drawn from its use (Messick, 1989; American Educational Research Assocation et al, 1999; Kane 2013). This is relevant to health care, where interventions are concerned with achieving a particular outcome. For example, where evidence-informed care is used, does it result in reduced interventions and improved outcomes, and how is the use of evidence to be supported so that positive outcomes can be achieved?
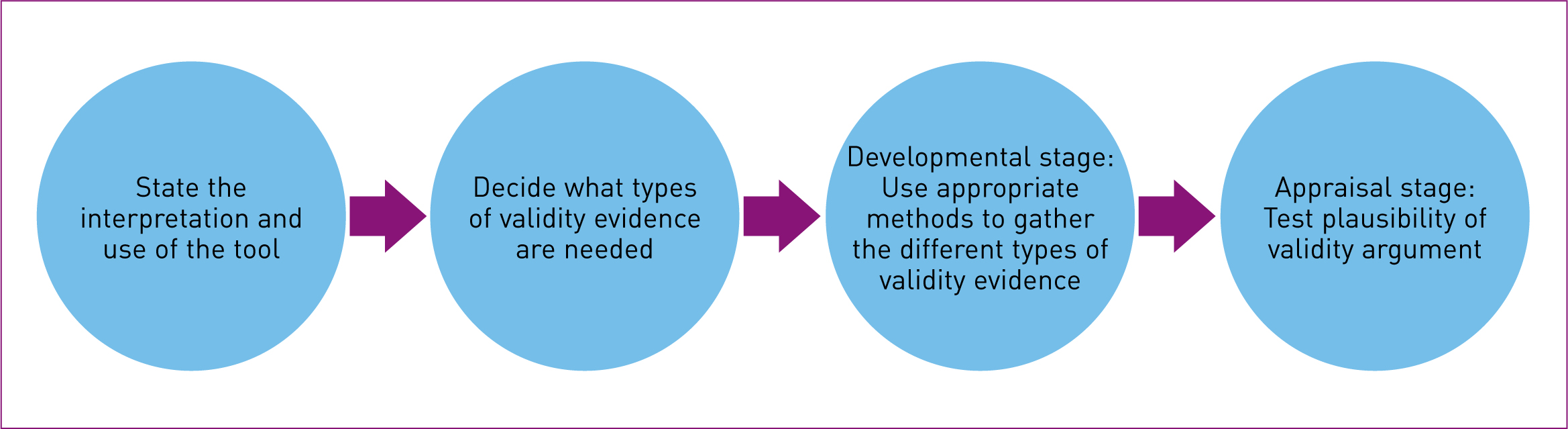
This framework is chosen because it offers a practical and easy-to-use guide on a complex process. It promotes an iterative process to maximise validity and reduce error from instrument design (Kane, 2013). There are two stages to the validation, a developmental stage and an appraisal stage. The validation of the KBN tool is in the developmental stage. This study aims to pilot the tool in the practice environment.
Aims
This study's objectives are:
The evidence gathered will be used to refine domains, items and rating scales prior to gathering validity evidence about content. The study will also explore the practitioners' experiences of using the tool in practice. This is particularly relevant to developing tools in health care, where usefulness and relevance—including how successful implementation can be achieved—must be considered prior to engaging in the lengthy and expensive process of validating a tool (Moore et al, 2015; Streiner et al, 2015a).
Ethical approval
The chair of the local Research and Development Office advised that National Research Ethics Service ethical approval was not required as the study did not involve NHS patients as participants. The risk of harm to women being cared for by a registered midwife with support from an experienced preceptor are minimal. The women were informed about the study by preceptors and no concerns were expressed. The midwife participants were fully informed about the study and were aware that they could with-draw participation at any time. Confidentiality and security of data were ensured in line with the Data Protection Act 1998 and Declaration of Helsinki 2008.
Methods and methodology
This study drew on pragmatism to inform its design. Pragmatism is often linked with practicalities associated with the ‘how to’ aspects of research and the use of mixed methods (Creswell and Clark, 2011). Morgan (2014) argues for a philosophical foundation to pragmatism. He draws on the work of John Dewey and notes that research is a process of inquiry based on thoughtful reflection informed by experience.
In gathering validity evidence, this study applied the philosophical underpinning of pragmatism by using practitioners and their experiences of using the KBN tool to inform the development of domains, items and scales, and strategies to promote successful implementation. It resonates with validity theory where processes are not purely focused on developing the properties of a tool but includes gathering evidence to support the interpretation and consequences from the use of the tool (Wolming and Wikström, 2010; Kane, 2013). Preceptorship offered the opportunity to pilot-test the tool. Preceptorship is not mandatory and the manner in which it is organised varies among Trusts (DH, 2010). However, it is an important process for targeting interventions to support implementation.
Mixed methods were used in this study (Creswell and Clark, 2011). A quantitative method was used to rate the relevance of domains to reducing unnecessary interventions and the usefulness of the tool. A qualitative approach was used to explore the experiences of preceptors and midwives who used the tool in practice; refine domains, items and rating scale; explore usefulness in greater depth; and identify barriers to implementation.
Sample
Midwives
All midwives (n = 35) involved in the care of labouring women at a local Trust were invited to participate in the study. Participants were sought via an email list. Flyers inviting participation were displayed prominently in all birthing environments. The consultant midwife identified several midwives who could benefit from participation, but recruitment from this group was unsuccessful. The final sample comprised three midwives from the birth centre and three midwives from the delivery suite (Table 3).
| Midwife | Current location | Experience |
|---|---|---|
| Midwife 1 | Birth centre (freestanding) | 1 year (delivery suite) |
| Midwife 2 | Birth centre (freestanding) | 1 year (delivery suite) |
| Midwife 3 | Birth centre (freestanding) | 6 months (delivery suite) |
| Midwife 4 | Delivery suite; moved to the birth centre after second evaluation | 6 months (delivery suite) |
| Midwife 5 | Delivery suite | 2 years |
| Midwife 6 | Delivery suite; dropped out after third evaluation | 2 years |
Preceptors
Midwives with expertise in working in the field of normal birth were invited (Table 4). Four had several years of experience working in a freestanding maternity unit and had regularly acted as preceptors. Apart from relevant practice experience, three were also involved in research into normal birth. Two were lecturers in midwifery and acted as preceptors on the delivery suite, where it was felt that piloting the tool without external preceptors would not be possible because of staffing shortages.
| Preceptor | Experience |
|---|---|
| Preceptor 1 | Senior midwife/researcher/PhD student/lecturer |
| Preceptor 2 | Senior midwife/researcher |
| Preceptor 3 | Senior midwife |
| Preceptor 4 | Senior midwife |
| Preceptor 5 | Senior midwife/midwifery lecturer/researcher |
Using the tool
Midwives began the process by assessing their practice with the tool. This was followed by five sessions in practice with preceptors, where the midwife's practice was assessed, supported, and progress measured by their preceptor. The portfolio at the end of the preceptorship included five rated practice sessions by the midwife and preceptor, five reflections on using approaches to reduce unnecessary interventions, and a record of practical application of these approaches.
Data collection and analysis
Midwives and preceptors who used the tool completed a questionnaire which had been previously piloted with two other researchers before use. It comprised statements about the relevance of the domains to reducing unnecessary interventions, the need for such a tool in practice and its usefulness in different categories of staff, and the provision of preceptorship to support implementation. It employed a four-point Likert-type scale ranging from ‘very useful’ to ‘not at all useful’. Quantitative data from the questionnaire were recorded on a Microsoft Excel spreadsheet and frequencies calculated.
Semi-structured interviews of 1-hour duration with five midwives and five preceptors were used to explore in greater depth all the elements contained in the questionnaire. The interviews were conducted at the participants' place of work, in privacy. All the participants were practitioners and known to the researcher, except for three midwives from the delivery suite. The interviews were audio-recorded and transcribed in full by the researcher. Raw data were stored in a master file and kept in a locked cabinet in the researcher's office. Data were entered onto a password-protected computer at the same location. Personal identifiers known only to the researcher were used to ensure anonymity while enabling communication for clarification, in line with the Data Protection Act 1998. The raw anonymised data were retained for future development of the tool and archived in a secure university database for a minimum of 5 years, complying with sponsorship guidance.
Data were analysed using thematic analysis. The researcher read the data several times, compared the data sets and colour-coded commonly recurring themes (Green and Thorogood, 2009). Specificity and frequency were noted. Under each theme, descriptive text was used to explore the theme, supported by quotes drawn from transcribed data (Mays et al, 2005). The data analysis and report were subsequently sent to all participants in the study for comments, and no disagreement was expressed (Mays et al, 2005).
Findings
Five midwives and four preceptors completed the questionnaire in full. One of the preceptors felt unable to use the Likert-type scale to rate the relevance of the domains.
Generally, the midwives and preceptors felt that the tool:
Three preceptors and one midwife saw the tool as ‘very useful’ for measuring practice, and two preceptors and four midwives felt it was ‘quite useful’. The midwives had been in practice for 6 months to 1 year before participation and explained that they would have benefited far more if they had used the tool soon after qualification (Table 5; Table 6).
| Midwives | Very useful | Quite useful | Not very useful | Not at all useful |
|---|---|---|---|---|
| Use in measuring practice | 1 | 4 | ||
| Use in student midwives | 5 | 0 | ||
| Use in newly qualified midwives | 4 | 1 | ||
| Use in experienced midwives | 1 | 3 | 1 | |
| Usefulness of preceptorship | 3 | 1 | 1* |
| Preceptors | Very useful | Quite useful | Not very useful | Not at all useful |
|---|---|---|---|---|
| Use in measuring practice | 3 | 2 | ||
| Use in student midwives | 3 | 1 | ||
| Use in newly qualified midwives | 3 | 1 | ||
| Use in experienced midwives | 2 | 2 |
Note: one preceptor rated the tool's use only in measuring practice; she did not feel comfortable using the rating scales and preferred to speak about her experiences
Midwives felt that interventions via preceptorship with the tool offered opportunities for reflection, critical discussions, writing about their experiences in reducing unnecessary interventions, and building confidence to implement evidence-informed skills. One midwife felt she would have benefited far more from the experience if she was supported by same preceptor throughout the pilot.
Of the three midwives who participated from the delivery suite, only one completed her participation there. Despite having been qualified for 2 years, she found the tool very useful. One moved to the birth centre after her second meeting with her preceptor, while another dropped out of the study.
One of the preceptors (P5) described the tool as ‘difficult to get to grips with’, particularly the use of the Likert scale to monitor progress. This preceptor felt that the scale of 0–4 did not adequately capture the development that had taken place; it was seen more as a tool to support and reflect on practice. The use of the tool to rate practice was questioned because of the many constraints on the ability of the midwife to use skills to reduce unnecessary interventions.
Refining domains, items and rating scale
All domains were scored highly for relevance to reducing unnecessary interventions, with a score of 7/10 or more (Table 7). One of the midwives wrote that domains where standards are often allowed to slip were 1, 2, 6, 7 and 12: philosophy, facilitating choice, supporting women in labour, progress in early labour, and respecting women. She hoped that ‘when the tool was used, these would be the areas that showed the greatest improvement or receive the highest rating’ (M1). The relevance of these domains was also scored highly by all midwives.
| Relevance of domains in measuring and supporting evidence-informed skills in Keeping Birth Normal, using scale of 1–10 |
Number of midwives |
Number of preceptors |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| 7 | 8 | 9 | 10 | 7 | 8 | 9 | 10 | ||
| 1 | Philosophy | 1 | 4 | 1 | 3 | ||||
| 2 | Facilitating choice | 1 | 1 | 3 | 1 | 3 | |||
| 3 | Guidelines | 5 | 3 | ||||||
| 4 | Environment | 2 | 3 | 2 | 2 | ||||
| 5 | Partnership working and communication | 1 | 1 | 1 | 2 | 1 | 3 | ||
| 6 | Supporting women in labour | 3 | 4 | ||||||
| 7 | Progress in early labour | 1 | 1 | 2 | 1 | 3 | |||
| 8 | Active labour | 2 | 1 | 2 | 1 | 3 | |||
| 9 | Imminent birth | 2 | 1 | 2 | 1 | 3 | |||
| 10 | Birth of placenta | 2 | 1 | 2 | 4 | ||||
| 11 | Birth of baby and breastfeeding | 2 | 1 | 2 | 1 | 1 | 2 | ||
| 12 | Respecting women | 1 | 4 | 1 | 1 | 2 | |||
Midwives and preceptors endorsed items in each domain as relevant to reducing unnecessary interventions, but felt that the number of items could be reduced because they were similar. Based on their feedback, items were reduced from 56 to 50.
Qualitative analysis of data from interviews
Four main themes were identified: usefulness and relevance, measuring practice, supportive relationships, and preceptorship.
Usefulness and relevance of the tool
All participants felt the tool was useful and relevant to measuring and providing support to keep birth normal.
‘ It was a good experience for the student midwife… an opportunity to be part of a team which allowed women to move from high-risk to as normal as possible ’
‘The tool is comprehensive. Its biggest strength is it enables us to speak concretely and objectively about reducing unnecessary interventions. Everything we do has a physiological impact. Breaking it down, assessing, identifying needs with plans to improve is fundamental to improving practice.’ (P1)
‘We went to work on the delivery suite. We changed everything around to create a good environment, dimmed light. It was good to know why I was doing what I was doing. This was not guesswork. The tool probes these discussions which I would not otherwise have with my preceptor.’ (M3)
For the midwives, the structured approach acted as a reminder to use evidence-informed skills. It presented an opportunity for reflection and created dialogue about the approaches being employed. It fostered confidence in the use of effective approaches; one midwife simply stated: ‘It works’ (M5).
The tool was described as particularly necessary in the delivery suite environment, where normalising birth is more challenging than in a midwife-led environment. Normalising birth in high-risk women was also identified as an important area for development using the tool. One midwife who was supported described the experience of using the tool among high-risk women:
‘It is a tool that can be used in all groups of women to reduce unnecessary interventions. It was a good experience for the student midwife as well and an opportunity to observe and be part of a team which allowed women to move from high-risk to as normal as possible.’ (M5)
This midwife felt confident after her participation in the study, ‘to not just to keep birth normal but also to challenge unnecessary interventions’.
Measuring practice
The five midwives in the study rated themselves highly in their reflection on practice. However, preceptors found that several items (approaches) needed further support and development. The midwives agreed:
‘After using the tool, I felt able to offer more options and better able to support women's choices. I was using some of the skills in the tool more than my colleagues on the delivery suite but on the birth centre it was deeper, a whole change in attitude to birth. There was a lot to reflect on…’ (M1)
This demonstrates the need for some form of peer or external assessment to develop expertise. Rating also allows the preceptor to provide specific support described by midwives as more useful, both in this study and in other work exploring experiences of preceptorship in practice (Hughes and Fraser, 2011). Two preceptors questioned whether rating could be discouraging to midwives who were newly qualified. There were concerns about the impact on practice by other pressures in their work environment. A softer rating, demonstrating a need for support, was suggested by one preceptor. Others felt differently, describing it as smart way to learn and needed in midwifery practice, where learning was very much ad hoc. One preceptor argued that formal assessments were an important part of improving standards; ‘such a tool would fill this gap’ (P3). Another said:
‘It is unacceptable for midwives not to be skilled in the items that the tool describes, or say they do not want to use such approaches. Can you say you do not want to do an epidural top-up? If you cannot say this, how can you say you do not want to do a water birth?’ (P1)
None of the midwives expressed concern about being rated. They understood that they were being supported to improve their skills and were glad to receive the support:
‘I knew what I did well and what I could do better next time.’ (M3)
However, it is worth noting that these midwives were a self-selected group who were keen to participate in the study.
One midwife described herself as having an ‘enhanced understanding of physiological labour and birth’ and another as ‘being supported to apply theory to practice’. This was evidenced in written reflections by the midwives and provided greater detail regarding specific learning that had taken place in relation to several items in the tool.
Supportive relationships
The midwives felt they needed the support of their preceptor, not only to implement approaches in the tool but also to receive reassurance that they were on the right path, and be praised and encouraged. Not all of them used the approaches the tool describes prior to qualifying or during their induction on the delivery suite.
Initial reflection on their practice prior to meeting their preceptors was particularly useful in helping them assess their own needs in a non-threatening way. Subsequent discussions and reflections with their preceptors and preceptor role-modelling of approaches were important facilitators of midwife learning:
‘I have witnessed how simple words said in the right manner helped my client calm down. I understood how good communication [and] close relationship with the client was important.’ (M5)
Preceptors felt working with the tool helped foster a relationship where the midwives felt more able to ask for support without feeling that they would be judged:
‘It can create a culture of open critique where the midwife can readily ask for help to improve their practice, communicate freely to learn…’ (P3)
Preceptors reported that the tool provided a platform for raising issues with midwives which they otherwise might not have done, particularly if they did not know the midwife or his/her practice. They were always conscious that they were working with a qualified practitioner.
The midwives felt better supported to develop their skills in the birth centre than on the delivery suite. They felt that even experienced midwives on the delivery suite lacked the ability to support their development in skills to reduce unnecessary interventions. All the preceptors and some midwives felt that senior midwives on the delivery suite could benefit from being observed and supported in their practice using the tool.
The midwives described their experience on the delivery suite as follows:
‘We were always coming up against people and situations that did not want us to keep birth normal.’ (M2)
‘They did not want to explore options. They said, this is how we have always done it. I was glad my preceptor was external or I would not have been able to do this. Sometimes it was easier to get support from obstetricians than midwives.’ (M5)
One of the midwives on the delivery suite felt bullied and unsupported within the unit, and withdrew from the study. The preceptor of the midwife who left the study said:
‘She moved from keeping birth normal to not engaging in these practices depending on the pressures put upon her. Often she was overloaded with work so she could not cope or be assigned to complex cases.’ (P1)
This midwife did not consent to an interview. Her preceptor felt the midwife still benefited from the three sessions in which she was involved. Another moved to the birth centre to continue her practice, and felt that this affected her ability to use the tool's approaches:
‘If I had not come to the birth centre, I would not be using the approaches the tool described. I was always confronted with “this is not how we do it here” and I did not feel able to stand up to this.’ (M4)
Both preceptors on the delivery suite found that such attitudes also interfered with their ability to support midwives. Midwives participating in the study were assigned to tasks that did not allow the use of the tool, despite coordinators being informed about their participation. They were assigned to high-risk women when the study required them to be assigned to low-risk women. Preceptors had to rearrange the planned engagement with midwives. One preceptor eventually decided to support her midwife by using the tool among high-risk women, with good results.
Preceptorship
Preceptors felt their ability to build relationships was affected by time allocated to other responsibilities. In the birth centre, this included antenatal, labour and postnatal work. Each shift was covered by just two midwives. On the delivery suite, problems included a lack of staffing, rostering that did not assign preceptors to their midwives, and a culture that did not view preceptorship as important to midwife development.
‘We were given a portfolio to complete but no one looked at it after this. We were expected to get on with it.’ (M2)
Both midwives and preceptors questioned the ability of midwives to act as preceptors and use tools that are not currently in use nor supported in midwifery.
‘The quality of preceptorship needs to improve. There is very little actual preceptorship that takes place. Midwives have become de-skilled in this area. You need competence in the use of the tool, be a competent practitioner as well as skilled in helping others knowing when to intervene and when to step back…” (P1)
However, there was optimism about the possibility of the tool creating a ‘snowball effect’ to develop a team of expert preceptors in normal birth in the future.
Discussion
This pilot study explored the usefulness and relevance of the KBN tool to measure and support the implementation of evidence to reduce unnecessary interventions. All participants felt that the tool was useful and relevant for this purpose. This was supported by the high ratings given to all the tool's 12 domains. The midwives felt it should be introduced soon after qualification for greatest benefit, but findings suggest introduction at any point can still offer benefits.
The tool promotes a closer scrutiny of midwifery practices to target specific support and improve outcomes. Ratings by preceptors challenged midwives' perceptions of the use of evidence-informed skills and created dialogue and reflection to improve implementation. There was a reluctance among some preceptors to rate practice because of perceptions that it is unfair in difficult work environments; it was suggested that the scale include a rating to denote need for support. However, a 5-point scale can result in bias from a reluctance to be critical (Streiner et al, 2015b). This reluctance was not universal, with some preceptors noting that such assessments were crucial to improving implementation. Such an approach is identified as needed in midwifery supervision and peer review processes (Alderwick et al, 2015; Kirkup, 2015; Royal College of Midwives, 2015).
A willingness to be assessed and supported is necessary to improve implementation. The lack of response to participation in the study by some midwives suggests that such willingness may not always be present. This may be related to cultural barriers to the implementation of such evidence in some birth environments. In their metasynthesis, O'Connell and Downe (2009) describe cultural obstacles to keeping birth normal, describing power and control exerted by senior midwives to ensure that other midwives subscribed to and complied with norms in the environment; this is evident in this study.
Midwives were questioned about using approaches to reduce interventions that were not commonly employed in the unit. Team leaders were not open to exploring options, preferring to intervene in the labour. Preceptors also encountered midwives who were obstructive in failing to assist those midwives who wanted to implement evidence or develop their skills, by not making opportunities to work with low-risk women available to them.
Midwives who felt unsupported on the delivery suite moved to the birth centre, where they believed they would be better supported to develop skills to reduce unnecessary interventions; this could be a reason why approaches to reduce interventions tend to be confined to midwife-led environments. However, as only 8% of women use such environments, this might be detrimental to improving outcomes (Birthplace in England Collaborative Group, 2011).
Kennedy et al (2010) identified a need for further research on midwifery practices that contribute to lower caesarean section rates and exploring why practice varies between environments. The KBN tool may permit such evidence to be gathered in the context of a mixed-methods study to include factors that act as barriers to implementation of these skills. This is important in promoting consistency of utilisation of such approaches across different birth environments.
One of the questions that this study raises is whether the use of the tool can develop midwives who are better able to resist dominant medicalised cultures on delivery suites. This is worth investigating, as most midwives work in large tertiary settings and reducing unnecessary interventions in delivery suites is important to ensuring positive outcomes for both low-risk and higher-risk women.
The successful implementation of such a tool requires expertise in approaches that reduce unnecessary interventions among midwives who act as preceptors. Investment in training is needed in the use of structured approaches that employ reflective models to support learning, and the use of rating scales and measures of progress to ascertain effectiveness.
In the birth centre, despite the availability of skills to reduce unnecessary interventions, lack of staffing and the organisation of work in the unit interfered with the ability to provide effective support. On the delivery suite, similar factors—along with a culture that did not promote normal birth—acted as barriers (O'Connell and Downe, 2009; Hughes and Fraser, 2011; NMC, 2011). This suggests the need for mandatory skilled preceptorship as a crucial intervention to ensure support for midwives in all birth environments, including protected time for such activity (DH, 2010).
The KBN tool requires and warrants further tests for validity and reliability prior to large-scale use: it has the potential to measure and support the development of expertise in keeping birth normal. However, its successful implementation in the context of preceptorship, and possibly other supportive peer relationships, will require commitment and investment in the education of midwives and leadership that challenges cultural barriers to promoting normal birth.
Study strengths and limitations
One of the main strengths of this study is the use of a framework to ensure a thorough application of validity theory to practice. The inclusion of practitioners who were known to the researcher and a keenness to promote a physiological approach may have resulted in response bias. The use of an iterative process that the Interpretation and Use framework promotes will addresses such biases (Kane, 2013). The next stage in this iterative process is content validation, where further validity evidence about domains and items using subject experts and women will be gathered.
This was a small study. On completion of the developmental stage, the tool will undergo plausibility testing using a larger sample. This promotes generalisabilty of the tool for large-scale implementation and validity of inferences drawn for its use.
Conclusions
All of the midwives in this study, whether newly qualified or experienced, felt they had benefited from structured preceptorship using the KBN tool. The tool provided a platform for measuring the use of evidence-informed skills, promoting dialogue and building a relationship that fostered role-modelling and reflection to promote implementation.
Staffing shortages, which reduce the opportunity to implement such formal and structured processes that facilitate support, need to be addressed. Organisations need to develop and support a culture of preceptorship in the clinical environment. This includes rostering and staff allocation during the course of a shift, assigning of midwives to supportive relationships and ring-fencing time for such activity. There is an urgent need for management to address a culture that is obstructive to approaches that normalise birth and penalises midwives who want to implement and develop such approaches.
In conclusion, this study shows that the KBN tool has the potential to be used in the context of the preceptor–midwife relationship to measure and support the implementation of evidence-informed skills to reduce unnecessary interventions. Other types of validity evidence about content, response processes and internal structure will need to be gathered prior to testing in a larger study before implementation. Successful implementation will require expertise in the use of approaches to reduce unnecessary interventions among preceptors in obstetric-led environments. Additional training in the use of rating scales, specific skills in role-modelling and critical reflection is also needed. The readiness of midwives to learn is fundamental. Investment in the use of structured approaches to improve implementation, supported by organisational cultures that promote normal birth, is crucial.